Pelvic Avulsion Fractures

Pelvic avulsion fractures are a unique injury seen almost exclusively in the adolescent population. At The Physios, it is one of the more common injuries we see in our younger patients. In this blog, we will explain what a pelvic avulsion fracture is, why they occur and how specialist paediatric physiotherapy can facilitate a full, safe return to sport. You can read more about other causes of hip pain in paediatrics here.
What is a Pelvic Avulsion Fracture?
A pelvic avulsion fracture occurs when a tendon or ligament pulls a small fragment of bone away from its main body. Unlike adults, whose tendons typically tear (a strain), adolescents have “growth plates” (apophyses) that are still developing. These areas of new bone are naturally weaker than the surrounding muscles and tendons. So a forceful injury that might cause soft tissue strain/sprain in an adult, often instead causes an avulsion injury in a child.
The most common sites for these injuries include:
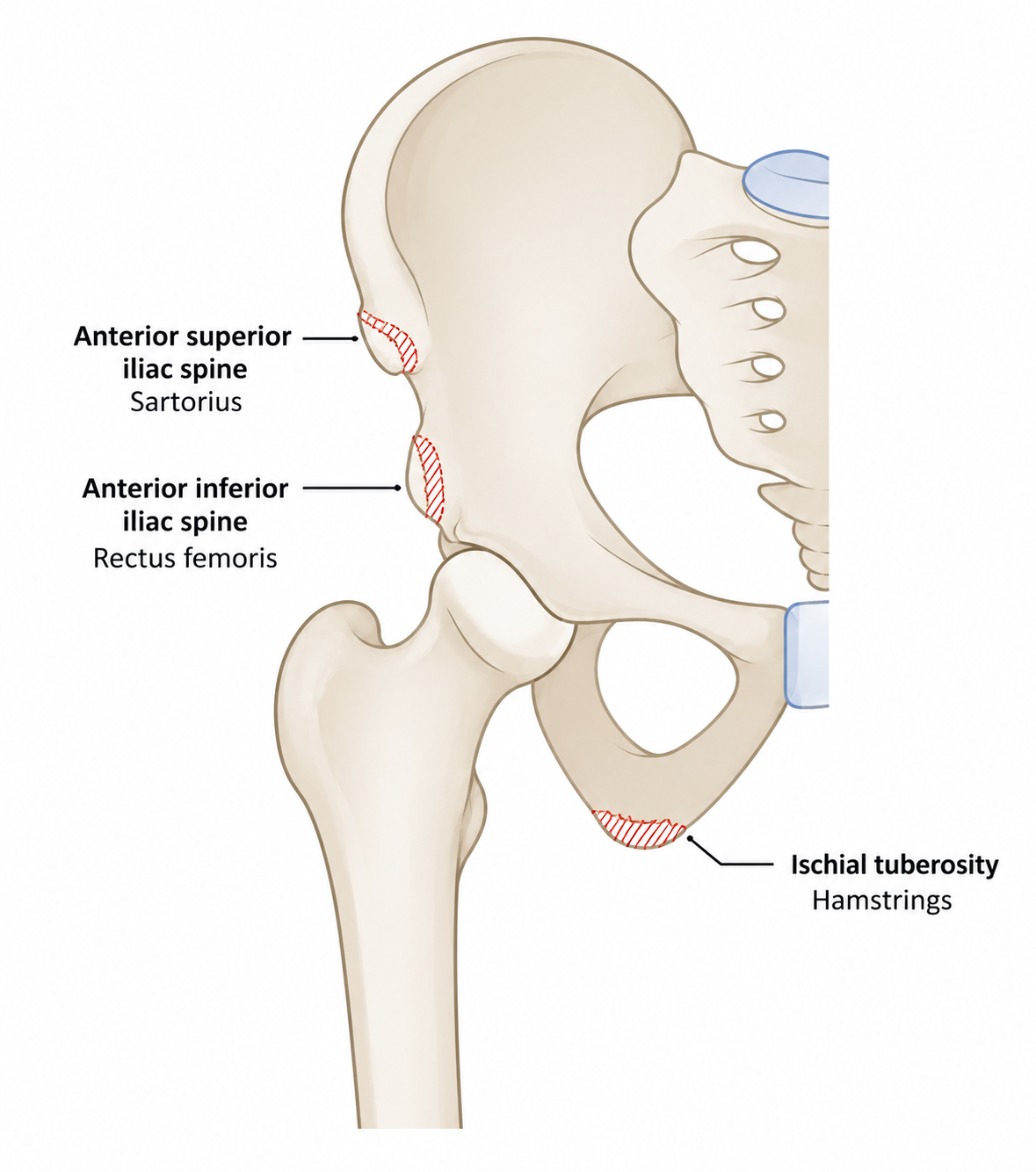
- Anterior Superior Iliac Spine (ASIS): Front of the hip, origin of the sartorius muscle
- Anterior Inferior Iliac Spine (AIIS): Just below the ASIS, origin of rectus femoris
- Ischial Tuberosity: The “sit bone” at the bottom of the pelvis, origin of the hamstring muscles
Who is Affected?
This injury typically affects adolescents aged 10 to 18 years. It is most common during the pubertal growth spurt when bones are elongating rapidly, and the apophyses (growth plates) have not yet fused to the rest of the pelvis. Research indicates a higher prevalence in males, who account for over 70% of reported cases.
How Do They Occur?
The typical mechanism is a sudden, forceful muscle contraction, often while the muscle is being stretched (an eccentric contraction). Common scenarios include:
- Sprinting or a sudden “take-off”
- Forceful kicking (e.g. football)
- Jumping or hurdling
- Sudden changes in direction
Patients often report hearing or feeling a sudden “pop” followed by immediate pain and difficulty walking or weight-bearing.
Diagnosis and Treatment
Diagnosis
A diagnosis is usually made through a combination of a clinical physical examination and X-ray imaging. Because the symptoms can mimic a simple muscle strain many injuries are initially misdiagnosed. This in turn can delay recovery. This is especially the case when children are assessed by clinicians who usually treat adults.
Treatment
The vast majority of pelvic avulsion fractures are managed conservatively (without surgery).
- Phase 1: Initial rest, ice, and protected weight-bearing using crutches for 2–4 weeks.
- Phase 2: Range-of-motion exercises and gentle activation work
- Phase 3: Progressive strengthening and return to sport drills
- Surgery: Only considered if the bone fragment is significantly displaced or in elite professional athletes
The importance of specialist paediatric physiotherapy
Adolescents are not just “small adults.” Their skeletal maturity and growth patterns require a nuanced approach. It is vital that they undergo rehabilitation with a physiotherapist who has specialist paediatric training. A specialist understands how to balance the demands of healing bone with the need to maintain strength, ensuring the athlete does not return to sport too early and risk a non-union or chronic pain.
Help your child get back to sport — pain free!
If your child is experiencing hip or pelvic pain that’s interfering with activity, we’re here to help. Contact our friendly reception team on 0114 2678181 to book an assessment with one of our paediatric physiotherapy specialists.







